
Abstract: This article explores how the models of medical risk from radiation established in the aftermath of the nuclear attacks on Hiroshima and Nagasaki are insufficient for understanding the risks faced by people in contaminated environments like Fukushima. These models focus exclusively on levels of external radiation, while the risk faced by people in areas affected by radioactive fallout comes from internalizing fallout particles. These models have helped to obscure the health impacts over the last 76 years of those exposed to fallout, from the people who experienced the Black Rain in Hiroshima, to the global hibakusha exposed through nuclear testing, production and accidents, and now to those living where the plumes deposited radiation in Fukushima.
Keywords: Fukushima, disaster, nuclear radiation, hibakusha, ecosystem, iodine, COVID-19.
When nuclear disasters happen, we look to past incidents to help us predict what human health impacts may follow, but not all radiological disasters are alike. The Three Mile Island, Chernobyl and Fukushima nuclear accidents were highly publicized and loom large in the public imagination, but these disasters are mere data points on a graph of nuclear incidents that have exposed the public to radiological harm. The “global hibakusha,” human beings that have been exposed to ionizing radiation, have suffered those exposures in multiple ways. The people of Hiroshima and Nagasaki are the only people to have been directly attacked by nuclear weapons. However, since then there have been more than 2,000 nuclear weapons detonated in tests. The communities downwind from those test sites did not suffer direct attack, but rather, were exposed to radioactive fallout from the mushroom clouds as they drifted. Besides the above listed nuclear meltdowns, multiple accidents have befallen nuclear reactors. Additionally, many people have been exposed to radiation through nuclear production at uranium mines, or plutonium production sites like Hanford. The disease toll from radiological exposure depends on the type of exposure. The most important distinction is between being exposed to radioactive waves that pass through your whole body, and radioactive particles that get inside your body and remain there. The biological routes are different and so the health outcomes also differ.
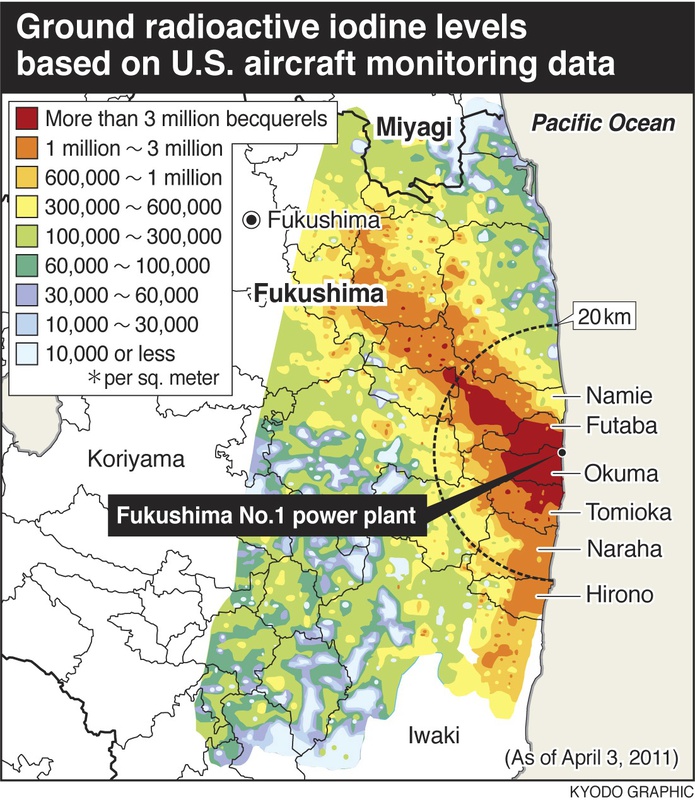
For the last 12 years I have been working on the Global Hibakusha Project, conducting field work in radiologically contaminated communities and populations all around the world (Broderick and Jacobs, 2018).1 As a historian, it is natural for me to think that looking to the past can help us imagine and anticipate the future. In April of 2015, four years after the Fukushima disaster, I gave a talk as part of the “4.11 International Symposium: From Hiroshima and Bikini to Fukushima and the World,” in Fukushima City. My lecture was titled, “Pretending Fukushima is New: How Studying Sites of Radiological Contamination Around the World Can Help Us to Understand the Present and Future in Fukushima.” The primary health risk that people in Fukushima face is from internalizing alpha-emitting or beta particles through inhalation, swallowing or abrasions. Yet predictions of their risks are almost entirely modeled on data from Hiroshima and Nagasaki where the exposures were predominantly from external gamma waves. This disconnect is visibly reflected to us in the maps of danger that always accompany discussions of the radiological legacy of Fukushima, maps like the one below. This application of data about external exposures to dismiss the health concerns of people immersed in a landscape dense with long-lived radioactive particles is not unique to Fukushima, it is elemental to how the majority of the millions of global hibakusha have remained invisible—have been rendered invisible.

Fig. 1: Radiation map showing both the distribution of radioactive iodine and concentric circles
radiating out from the site of the Fukushima Dai’ichi Nuclear Power Plants (Kyodo)
My chapter in Legacies of Fukushima: 3.11 in Context, “Fukushima Radiation Inside/Out,” argues that the maps of contamination we use to understand the risks downwind from the Fukushima Daiichi plant are flawed. They model a pattern of danger and safety that works as hard to obscure certain dynamics as it does to delineate others. These broken maps reflect health models about harm from radiation that are limited yet invariably presented as inclusive and comprehensive.
As mentioned above, we biologically encounter radiation in two distinctly different manners. Our whole bodies are exposed to radioactive rays when we are immersed in high levels of radiation that are external to our bodies, as happened in Hiroshima and Nagasaki. The detonations of those weapons released high-energy gamma and neutron waves that were similar to a single giant x-ray that penetrated entire bodies and extended out several kilometers from the hypocenter. Separately from this form of exposure is when we encounter radionuclides, individual radioactive particles that remain after nuclear detonations, either as beta particles or alpha-emitting particles. We often refer to radiation in this form as “radioactive fallout” since it usually deposits into our ecosystems by “falling out” of clouds drifting from radiological explosions or fires. Once the particles have dispersed into the ecosystem, they are harder to locate. These are primarily dangerous to us if we internalize them inside of our bodies. If they remain inside of our bodies, they emit their very small amounts of radiation to nearby cells 24 hours a day for however long the specific particle remains radioactive. For some particles that is days, for many it’s centuries or longer. Cesium-137, a particle that spread in large amounts after both Chernobyl and Fukushima, remains dangerous to living creatures for 300 years. These two forms of exposure (external whole body vs. internalized in a specific bodily organ) present distinctly different risks to human health (for a primer on these forms of radiation see here).
The risks that people downwind from the Fukushima plants face is primarily from fallout. Large amounts of fallout can also present danger from their collective external radiation when they first deposit, however, now, 10 years later, those particles have distributed into the ecosystem. Settling into soil, moving with rainwater and groundwater, being taken up by plants and animals: they are embedding and migrating. As they spread out, our ability to detect them degrades. Since Geiger Counters measure the external energy that the particles radiate, we usually find them when they are present in large amounts. Now that they are widely dispersed, many have migrated far from the color-coded maps of risk we see of Fukushima. Those maps are snapshots of external readings at a specific moment that has passed.
In Fukushima, relatively few people are being exposed to high levels of external radiation except for the cohorts of onsite workers at the nuclear plant site, those involved in decontamination efforts, and those who lived where the fallout deposited in large amounts. People living in most (but not all) of the areas where heavy fallout deposited were evacuated fairly quickly. For those who continue to live in, or are being returned to areas of lower contamination, we still measure the external levels of gamma radiation to predict the risks they face. However, just as with the Marshallese after US thermonuclear testing, just as the Kazakhs after Soviet testing, and just as with those living in contaminated areas downwind from the Chernobyl plant in Ukraine and Belarus, the primary risk to the public health is not the external radiation, the primary risk is that one may internalize radioactive particles and retain them inside the body. Telling someone that the external levels of radiation are not high is not actually saying that they are not at risk, it is just a way of saying that we only have models that delineate risks from the external levels. And if those are low, we declare, health agencies declare, UN public health bodies declare: there is no significant risk. Yet there is. Those living in contaminated regions of Fukushima join a long list of people whose homes and communities have received significant deposits of radionuclides through fallout. All have invariably had their levels of risk minimalized. Many have had their anxieties cited as irrational and pathologized as “radiophobia.”2 Almost none have received any compensation for their health problems and the loss of value of their lands and businesses.3
In Fukushima, as downwind from nuclear test sites, communities experienced large deposits of radioactive fallout, yet the model that has always been used to predict health outcomes is based on studies of Hiroshima and Nagasaki: this is the wrong model for these disasters. In Hiroshima and Nagasaki there was a massive burst of external radioactive gamma and neutron waves at the moment the nuclear weapons detonated, lasting less than a minute. This was followed by radioactive fallout as the mushroom clouds deposited radioactive particles (beta and alpha-emitters) and drifted.4 The health models built out of Hiroshima and Nagasaki only assessed the harm from the external exposures. These models emerged from studies done at the Atomic Bomb Casualty Commission in Hiroshima and Nagasaki since 1946 (reformed in 1975 as the Radiation Effects Research Foundation), especially the Life Span Study (LSS) which began in 1950. This study establishes a large database, corelating radiation exposures to subsequent health outcomes and early mortality. The study is rigorous, yet its use in the years since Hiroshima and Nagasaki has frequently been careless. The LSS assesses only external radiation exposures, it explicitly excludes consideration of the health effects of internal radiation exposures from living with fallout. There is nothing wrong with this methodological choice. Hiroshima and Nagasaki were events in which a large cohort of people were exposed to a single large dose of external gamma radiation. It would have been very difficult at the time to determine who had internalized a radionuclide and who hadn’t. In the early years of the Cold War, it was assumed that future wars would involve the use of nuclear weaponry and the exposure of many people to large bursts of gamma rays as were the people near the hypocenter of Hiroshima and Nagasaki. But that was not what happened; instead, over 2,000 nuclear weapons were tested, and millions of people were exposed to radioactive fallout. We did not have a robust database on the health consequences that might result from these exposures—so we used the tool we did have, the LSS. The LSS tells us little about the risks faced by people living with large depositions of fallout.
The Cold War period, and beyond, are periods in which the invisibility of the health consequences of exposures of internalized radiation was made invisible, and the misapplication of the LSS was elemental to this cloaking. A key reason that the LSS has been weaponized to obscure the health effects of internalized radiation exposures is that since the exposures did not happen as acts of war, but rather as weapon development, those exposed should be entitled to compensation for their health problems, and the loss of value to contaminated land. This would likely have restricted nuclear weapon testing. These dynamics have been extended to obscure and shield compensation obligations in other historical instances of large-scale radiological contaminations such as waste dumping and nuclear accidents.
All of us have been dealing with the horrors and the terrors of the COVID-19 pandemic since early 2020. Viscerally, we feel the anxieties and fears that accompany uncertainty about dire risks to our lives and loved ones. Being cautious about our public activities in the age of COVID makes intuitive sense. We navigate our potential exposures, work to mitigate our potential contaminations, and worry endlessly about loved ones with health concerns. Each small, unrelated medical symptom a family member exhibits is met with anxiety. This is a reality for people worldwide. Those who live in areas dense with radionuclides face similar anxieties: the locations of the risk are indeterminable; who is being exposed and who is safe is unclear, even while the damage is inflicted; daily life is rife with anxiety. But in radiologically contaminated communities it is not conspiracy theorists on social media dismissing them as irrational, it is state health officials. They draw maps, based entirely on externally measured levels of radiation, and use those maps to tell people to move back to villages where the levels of contamination are “acceptable,” to send their children to schools and move back to towns where the presence of radioactive particles is not dense enough to register on Geiger counters placed high above the ground.

Fig. 2: Fixed station radiation monitor post.
Imagine a map of COVID cases that shows high levels in one city and low levels in the adjoining city, and being told that therefore there is no risk at all once you enter the city with lower levels. We would all continue to be cautious. That is common sense, not (radiophobic) irrationality. If a group of 10 people were to stand downwind from someone coughing out COVID microbes, some may get sick and some may not. Who has inhaled a microbe and who hasn’t will not be visible until the disease presents. This is what it is like to live in an ecosystem with migrating radionuclides. Even if their presence is not significant enough to make a Geiger counter ping, caution is rational. However, the history of fallout contamination is a history of dismissing the health concerns and worries of the populations living in the areas where fallout came down.
A clear way to visualize how the reliance on external measurements to determine risk is problematic is to examine the scientific literature on Fukushima. Biologist Timothy Mousseau, with colleague Anders Møller, has conducted field work in the Zone of Exclusion in Chernobyl for decades (primarily on birds and small insects for whom multiple generations of inheritance have passed), and have sought to conduct corollary field studies in the evacuation zones of Fukushima. Speaking to an IPPNW symposium on the 10th anniversary of Fukushima, Mousseau examined the top 500 articles in the Web of Science database. He found that only 10 out of the top 500 papers (2%) were based on actual biological fieldwork assessing the impacts of radiation on living organisms. Almost all of the other 98% were studies of “calculated doses and the possible link to health impairments rather than any sort of directly measured biological consequences” (Mousseau, 2021).5 Most of the scientific literature around Fukushima, and Chernobyl, are based on estimates of health impacts utilizing externally measured radiation and applying statistical models such as the Life Span Study. These estimates are not observed findings, but predictions of the numbers of cancers and early mortality that may be expected in the future among the exposed population.
This model of utilizing measurements of external radiation and statistical databases of disease probabilities has been a critical component of how the global hibakusha have been ignored since the advent of nuclear weaponry. As radioactive fallout blanketed communities downwind from the Nevada Test Site, and other nuclear test sites around the world, such assessments were routinely used to dismiss the health concerns of downwinders. Now, many of those same individuals (in America) whose health concerns were dismissed are recipients of Radiation Exposure Compensation Act funds from the US government. Ignored and dismissed for decades because of the use of external modeling and statistical correlation of that modeling to the LSS, select members of these communities were only able to obtain recognition and some small compensation late in their lives because they were full citizens with access to legal remedies in a wealthy nation.
As I detail in my forthcoming book Nuclear Bodies, nuclear test sites are not chosen because of their scientific properties, rather, communities are selected to be irradiated because of their political inability to resist such treatment. Nuclear test sites are built upwind of these communities. Hence, most of the exposures of global hibakusha were in colonial or postcolonial spaces, or were citizens of poor or developing nations and have not been recognized or awarded compensation for their suffering.6 Their subaltern political status was fundamental to their communities being chosen as radiologically disposable. For example, the British and French never tested nuclear weapons within their own national borders. Along with the United States, the British and French tested all of their thermonuclear weapons (hydrogen bombs that yield vastly larger fallout clouds) in Pacific nations either directly under their control, or of actual colonial status (specifically, the Marshall Islands, Kiribati and French Polynesia). Keeping these big fallout clouds outside of their own borders was national policy to protect their own populations, and conversely, put them inside the borders of other nations and subjected their populations to risk. This has never been accidental. Nuclear power plants are not sited inside of the urban areas where their electricity is consumed, but in the rural areas at a distance so that if there is a radiological release it exposes less people, but also less politically powerful people. Kate Brown has cited how the Soviet government purposefully seeded clouds from Chernobyl to rainout their particles in Belarus rather than over the large Russian cities they were drifting towards.7
Relying exclusively on maps of externally measurable radiation and medical models based solely on the harm caused by external exposures extends this invisibility for further generations and will continue to legitimize dismissing and ignoring both the health and emotional impacts of radiation exposures into the future. Fukushima is part of a continuum of the dismissal of the harm endured by those who suffer from internal exposures to radioactive particles from nuclear tests, nuclear accidents and nuclear production worldwide. Looking at the broken maps works to obscure the real risks in Fukushima.
Many of the particles embedded in the ecosystem of Fukushima will remain dangerous to living creatures for hundreds, or even thousands of years. During this period, they will not stay put. As I point out in my chapter in Legacies of Fukushima: 3.11 in Context, this reveals the decontamination theater of soil removal in Fukushima. The years since 3.11 have seen a continual media presentation of crews removing radioactive topsoil from towns, schoolyards and homes in Fukushima.

Fig. 3: Decontamination crew works to decontaminate a roadside in Iitate in 2015 (Greenpeace).
Almost certainly the particles in the forest canopy and on the trees will re-contaminate this roadside within a year.
The reduction in radiation levels is the predicate for declaring towns safe for return. The particles themselves remain radioactive; the fields filled with plastic bags of particles stacked around the region are now nuclear waste sites that must be managed for generations. The theatrical aspect is in pretending that by removing the radioactive particles from the towns they are now “clean.” Since the towns are themselves situated in larger ecosystems full of radionuclides, this “decontamination” cannot last: wind, rain, typhoons will all strip particles down from the forests and mountains surrounding the towns and re-contaminate them. Similar to how the Tokyo 2020 Olympics were meant to produce the impression that Fukushima has recovered, all theater requires the willing suspension of disbelief. When we placed a containment dome over the melted core of Chernobyl reactor unit #4 people assumed that the Chernobyl disaster was clearly over, only to be surprised to read in the papers about ongoing criticalities in the subterranean core that threatened ongoing releases. Long-lived particles create ongoing and fluctuating realities. Fukushima is not simply something that happened, it is something that is still happening.
References
Broderick, M. and Robert J. (2018) ‘The Global Hibakusha Project: Nuclear post-Colonialism and Its Intergenerational Legacy’, Unlikely: Journal for the Creative Arts, 5 [online]. (Accessed: June 5, 2021).
Brown, K. (2019) Manual for Survival: A Chernobyl Guide to the Future. London: Allen Lane.
Jacobs, R. (2013) ‘Nuclear Conquistadors: Military Colonialism in Nuclear Test Site Selection During the Cold War’, Asian Journal of Peacebuilding, 1(2), pp. 157-177.
Mousseau, T. 2021. “Ecology in Fukushima: What Does a Decade Tell Us?” [Online video]. (Accessed June 5, 2021).
Petryna, A. (2013) Life Exposed: Biological Citizenship after Chernobyl. Princeton: Princeton University Press.
Stawkowski, M. (2017) ‘Radiophobia Had to be Reinvented’, Culture, Theory and Critique, 58(4), pp. 357-374.
Notes
The outcomes of this research will be published next year in, Robert Jacobs, Nuclear Bodies: The Global Hibakusha (New Haven: Yale University Press, 2022), forthcoming. Also, see my blog Global Hibakusha.
The areas where fallout came down most heavily downwind of Hiroshima is referred to as being affected by “black rain,” this is because rain strips fallout particles from the air and brings them down in large quantities, and the black soot from the fires in Hiroshima made the rain black and sticky. The rights of those who suffered illness from exposure to black rain, and also from exposures resulting from entering the city in the weeks after the nuclear attack, are still being litigated and contested in Japanese courts today.